New Telehealth Guidance
Throughout the Covid-19 pandemic, HHS (the US Department of Health and Human services) has released guidelines on telehealth services and audio-only visits for patients to meet with their healthcare providers. Due to the eventual conclusion of the pandemic, HHS has released the newest guideline for maneuvering through the latest changes.
Healthcare providers and entities that are covered under insurances may continue to offer telehealth and audio-only visits to their patients as long as it still follows HIPAA regulations. While access to some telehealth services may be more complicated for some, audio-only services that do not required broadband availability are still accessible. This guidance addresses these concerns and whether or not audio-only telehealth is permissible under HIPAA regulations. HIPAA requires safeguards to prevent any potential incidental uses or disclosures of a patient’s private information. For example, telehealth and audio-visits are expected to be held in private settings; if not in private-enough settings, at least they should be performed discreetly. “The Telehealth Notification provides that OCR will exercise its enforcement discretion and will not impose penalties on covered health care providers for noncompliance with the requirements of the HIPAA Rules in connection with the good faith provision of telehealth using non-public facing audio or video remote communication technologies during the COVID-19 PHE. As such, under the Telehealth Notification, covered health care providers can use any available non-public facing remote communication technologies for telehealth, even where those technologies, and the manner in which they are used, may not fully comply with the HIPAA Rules. The Telehealth Notification will remain in effect until the Secretary of HHS declares that the COVID-19 PHE no longer exists, or upon the expiration date of the declared PHE, whichever occurs first,” (HHS, 2022). Along with protecting the patients PHI, providers also have to keep in mind their accessibility to those with disabilities. This includes effective communication, which may result in auxiliary aids and language assistance, just to name a few. Covered healthcare providers may continue to offer telehealth and audio-only services that coincide with HIPAA rules and regulations, regardless of the patient’s insurance and whether or not their health plan pays for those services.
For more information, please visit HHS.GOV.
Source:
(OCR), Office for Civil Rights. “Guidance: How the HIPAA Rules Permit Covered Health Care Providers and Health Plans to Use Remote Communication Technologies for Audio-Only Telehealth.” HHS.gov, 10 June 2022, https://www.hhs.gov/hipaa/for-professionals/privacy/guidance/hipaa-audio-telehealth/index.html?mkt_tok=MTQ0LUFNSi02MzkAAAGFC18_eMVv9V_yJW9oZ7kIljmgJJr4T6BGnZS1XJlgD0EfdSV2MU6oCTmkDXuD6Rq1Cdu0fu7STPWafVTsKForEg1iEMFQnk4ezzV4LVhrxA#footnote1_ahe58oj?utm_source=nl-gov-ed-washington-connection-2022-06-16&utm_medium=email&utm_campaign=government-affairs.
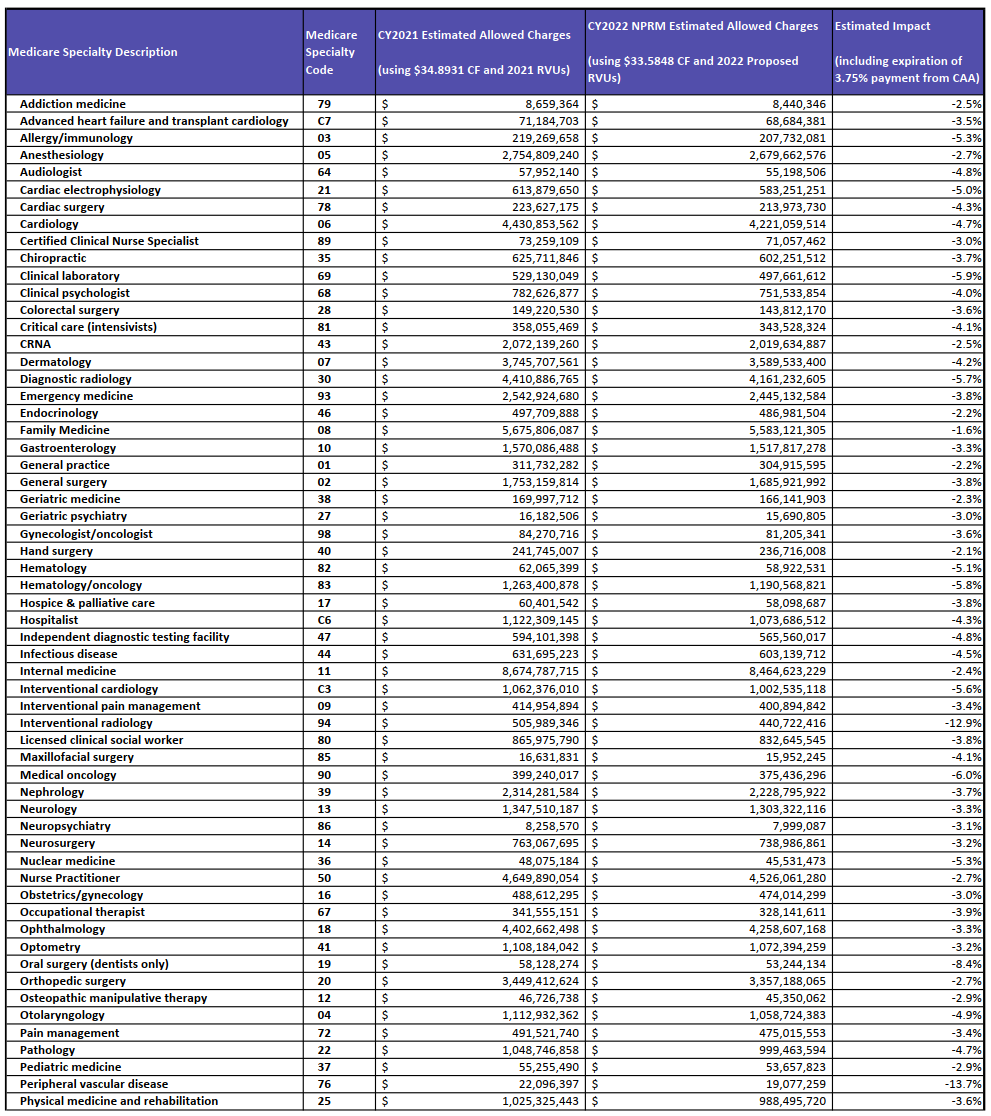
The 2022 calendar year physician fee schedule for Medicare physicians includes new proposals that may prove to be complex and intricate; these proposals can significantly impact group and individual practices starting as soon as January 1, 2022. The proposals will affect physician reimbursements, as well as quality reporting guidelines. Included in these are policy proposals that will update the annual conversion factor; “The conversion factor is the multiplier that Medicare applies to relative value units (RVUs) to calculate reimbursement for a particular service or procedure under Medicare’s fee-for-service system,” (Frieden, 2021 Medicare Fee Schedule). These proposals will also make changes to covered services that are rendered under telehealth, change the definition of what a shared visit looks like, and present the “Merit-based Incentive Payment System Value Pathways” as an option for reporting for the 2023 calendar year.
It is estimated that the conversion factor will decrease in amount from the previous year; $1.31 to be exact. Many physician organizations are working together to try and find a solution to these cuts before they are put into effect. Please see the charts below to see how this can affect your specialty.
Continuing on with payment for those telehealth services that were temporarily placed on the telehealth services list, CMS has granted an extension until the end of 2023. Normally, changes to telehealth billing guidelines are restricted to adhering to the list of covered telehealth services. However, due to the public health emergency (PHE) Covid-19, CMS has allowed flexibility. Changes to mental health services are being added to the list, allowing the patients’ home to be a place of rendering services as long as the patient has been seen in-person within the last 6 months. Following that, as long as the patient has been seen within the last 6 months, audio-only visits can be covered as well. The Covid-19 PHE has changed healthcare long-term by allowing more options for services to be rendered; as such, CMS has permanently approved covering the code G2252: brief communication via technology between the patient and physician or other qualified health care professional.
“A split/shared E/M [evaluation and management] visit is defined by Medicare Part B payment policy as a medically necessary encounter with a patient where the physician and a qualified NPP each personally perform a substantive portion of an E/M visit face-to-face with the same patient on the same date of service,” (AAPC, Medicare Policy). CMS intends to change this definition to reflect NPPs (non-physician practitioners) and their role in the health field. This proposal changes how these E/M visits can be billed by each health care professional, which visits can be billed, and which patients can be billed (established patients versus initial visits). Documentation has also been added to; the medical record must show both of the healthcare professionals that performed the visit, and the practitioner that performed a majority of the visit must sign and date the record.
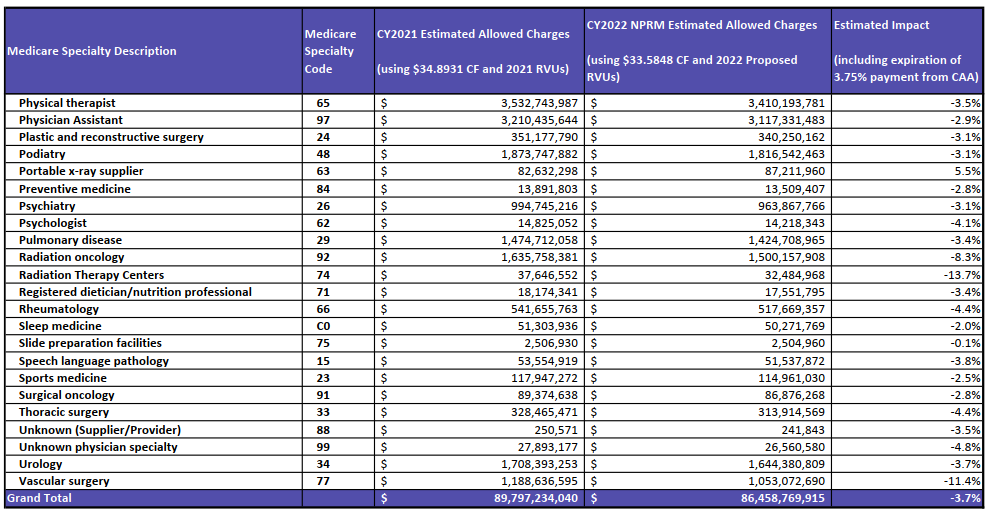
CMS plans to increase the amount of specialties on the list of eligible clinicians for MIPS; this is including social work and certified nurse-midwives, and the performance category will automatically be reweighted to account for this change. This change not only affects those in social work and midwifery, but all group and individual practices; reweighting will impact those practices that have already been included on the MIPS list. Please click the links below to view the estimated impact on your specific specialty.
View the Medicare Specialty Description Amount Image 1
{kind=link}
View the Medicare Specialty Description Amount Image 2
{kind=link}
Sources:
Aapc, Admin. “Medicare’s Split/Shared Visit Policy.” AAPC Knowledge Center, 1 Aug. 2008, www.aapc.com/blog/23741-medicares-splitshared-visit-policy/#:~:text=1.,the%20same%20date%20of%20service.
Frieden, Joyce. “2021 Medicare Fee Schedule Includes 10.2% Cut in Conversion Factor.” Medical News, MedpageToday, 2 Dec. 2020, www.medpagetoday.com/practicemanagement/reimbursement/89970.
Yeo & Yeo Medical Billing & Consulting is pleased to announce that Denise Garrett has earned the Certified Outpatient Coder (COC) credential recognizing her expertise in outpatient hospital and ambulatory surgical center coding.
 To earn the credential, Garrett passed the COC exam, validating her expertise in medical terminology, anatomy, payment methodologies, compliance, ICD-10-CM, CPT and HCPCS Level II coding, surgical coding, and modifiers.
To earn the credential, Garrett passed the COC exam, validating her expertise in medical terminology, anatomy, payment methodologies, compliance, ICD-10-CM, CPT and HCPCS Level II coding, surgical coding, and modifiers.
Garrett is an account manager and has more than 20 years of medical billing and coding experience. In January of this year, Garrett was appointed to a three-year term on the American Academy of Professional Coders Chapter Association (AAPCCA) national board of directors.
Garrett is a Certified Professional Coder (CPC), Certified Physician Practice Manager (CPPM®), Certified Professional Compliance Officer (CPCO™), Certified Professional Medical Auditor (CPMA®), and a Certified Surgical Foot & Ankle Coder (CSFAC), with expertise in the coding of diagnoses, services, and procedures for physician practices. She is also a member of the American Medical Billers Association (AMBA), the American Institute of Healthcare Compliance, the National Alliance of Medical Auditing Specialists (NAMAS), and the American Association of Medical Coding Professionals (AAOMCP), and is a board member for the American Academy of Professional Coders (AAPC) Bay City Chapter.
Health and Human Services (HHS) announced its overview of reporting requirements for healthcare providers who received any of the COVID-19 CARES Act Provider Relief Funds.
Any provider who received one or more payments exceeding an aggregate amount of $10,000 will be required to report how the funds have been used.
Detailed instructions regarding what and how to report will be released by August 17. Also, HHS will provide a question and answer webinar before the reporting deadline to ensure all providers can adequately account for the use of funds for allowable purposes, for each Provider Relief Fund payment.
Timing of reports
The reporting system will be available to recipients for reporting on October 1, 2020.
- All recipients must report within 45 days of the end of calendar year 2020 on their expenditures through the period ending December 31, 2020.
- Recipients who have expended funds in full before December 31, 2020, may submit a single final report at any time during the window that begins October 1, 2020, but no later than February 15, 2021.
- Recipients with funds unexpended after December 31, 2020, must submit a second and final report no later than July 31, 2021.
- Detailed Provider Relief Fund reporting instructions and a data collection template with the necessary data elements will be available through the HRSA website by August 17, 2020.
Read the full HHS notice. Yeo & Yeo will send an update once the reporting requirements are released.
Yeo & Yeo Medical Billing & Consulting is pleased to announce that Denise Garrett has completed the required training to become a Certified Healthcare Auditor (CHA).
To earn the certification, Garrett needed to pass a course designed by the American Institute of Healthcare Compliance and be an advanced and certified coder. Garrett’s expertise will benefit the company’s healthcare clients as she focuses on critical areas of audit compliance, how to perform gap analysis, and creating forms to use during the audit process.
Garrett is an account manager and has more than 20 years of medical billing and coding experience. She is a Certified Professional Coder (CPC), Certified Physician Practice Manager (CPPM®), Certified Professional Compliance Officer (CPCO™), Certified Professional Medical Auditor (CPMA®), and a Certified Foot & Ankle Surgical Coder (CFASC), with expertise in the coding of diagnoses, services, and procedures for physician practices. She is also a member of the American Society of Professional Coders, the American Medical Billers Association (AMBA), and the American Institute of Healthcare Compliance, and is a board member for the American Academy of Professional Coders (AAPC) Bay City Chapter.